Pressure


Flow and Pressure on the EDM+
The EDM+ brings together the minimally invasive esophageal Doppler monitoring of blood flow with a pulse pressure wave analysis (PPWA) system.
Esophageal Doppler is the gold standard for measuring change in cardiac flow and making clinical decisions.
It is not necessary to have an arterial line to monitor cardiac function using Doppler, however, easy calibration =of the EDM+ arterial signal provides continuous monitoring of Cardiac Output (CO). This may be useful if the Doppler signal is unavailable during electrocautery.
EDM+ also offers the combination parameters of Cardiac Power Output (CPO) and Cardiac Power Index (CPI)

Blood Flow with Arterial Pressure

Pressure Monitoring Mode

Connect your existing patient monitor to the EDM+ via the ADC jack plug on the back.
This feeds your existing arterial signal into the EDM+ to provide pressure information.
Once you have an optimized Doppler signal, arterial pressure can be calibrated at the touch of a button.
See the transfer Cable guide for EDM+
The Arterial Waveform


Pressure measurements taken further away from the aorta are characterized by:
- A taller systolic peak
- A deeper dichrotic notch
On the EDM+ monitor the arterial wave is scaled to an appropriate size for comparison with the Doppler waveform.
Using Flow or Pressure Monitoring Mode


Use Flow Monitoring Mode for direct measurement of flow and to guide interventions.

Use Pressure Monitoring Mode:
- if the Doppler signal is unavailable e.g., during electrocautery
- for continuous monitoring
- for post-operative monitoring of an awake patient
If pressure monitoring continues after the Doppler probe has been removed, you will be prompted to recalibrate if the signal deviates by 20% or more. It is then a clinical decision whether to use an ‘awake probe’ (the softer more flexible I2C) for calibration or to sedate the patient and use a standard probe.
How Deltex Medical Derives CO from Arterial Pressure

Research and development for the EDM+ evaluated 9 available algorithms that convert pressure to flow parameters.
The Liljestrand and Zander method was chosen because it proved superior to the other algorithms, especially during changes in compliance.1-3
1 Caillard et al. BJA 2015;114:893-900.
2 Monge Garcia et al. Critical Care 2013;17:R113.
3 Sun et al. Crit Care Med 2009;37:72-80.
When do I Calibrate
Any known or suspected change in arterial compliance is an indicator for recalibration.

Arterial compliance is an index of elasticity:
– calculated from change in blood volume for a given change in blood pressure (BP).
- Changes in arterial compliance can affect the amplitude and shape of the arterial pressure waveform.
- Vessels become less compliant (elastic) with increasing age
- Acute changes in arterial compliance commonly occur during surgery due to interventions such as:
- Anesthesia
- Other vasoactive drugs
- Physiologic responses to stimuli
Pressure Monitoring

When any arterial line is used to measure pressure there are three factors that influence the accuracy of the signal:
- Leveling
- Zeroing
- Damp testing
These should be done before using the arterial signal on the EDM+ and should be checked whenever there is doubt about the arterial signal.
Leveling
Influences accuracy of all arterial lines
The arterial cannula forms a closed fluid system with the body where we are measuring the force (or height) of a column of water (the tubing) above the transducer. This measurement changes with positioning.
The right atrium is a suitable reference for leveling the transducer. This is located approximately at the intersection of where a line from the fourth intercostal space at the right side of the sternum (A) meets the midaxillary line (B) – the phlebostatic axis.
- Invalid if the patient has a barrel shaped chest or severe chest deformity.

A consistent angle is best for measuring pressure trends.
This measurement can be taken with the patient supine or raised to a 60˚ angle.
Note: changes in the angle of the bed after leveling may give a false result.
- At set up of arterial line and prior to using EDM+
- At handover
- When any doubt exists about the arterial readings
- Whenever patient position is altered, the transducer height should be altered.
Zeroing
Influences accuracy of all arterial lines

Atmospheric pressure is a constant in the room. Just as weighing scales can be set to zero, atmospheric pressure can be eliminated from the readings by exposing the column of fluid to the pressure in the room. This requires the 3-way tap to be closed to the patient. A value of ‘zero’ can then be set on the monitor.
This is usually performed:
- At set up of arterial line and prior to using EDM+
- Once per shift, or at handover
- After being disconnected from patient’s main monitor
- When any doubt exists about the readings
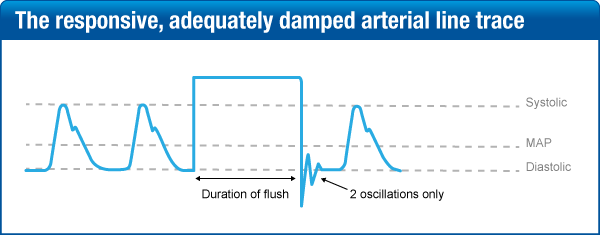
Damp Testing (Square Test)
Influences accuracy of all arterial lines
This test is designed to evaluate vibration detected by the transducer and the degree to which it is restrained or damped.
When the flush valve is opened and fluid is pushed quickly through the giving set, a square wave is created in response on the arterial trace on the patient’s main monitor. The degree of oscillation detected by the transducer after the flush reflects the degree of damping in the system.
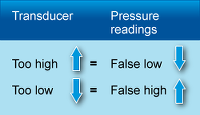
Damping – Too Much or Too Little?
Too much variation is observed when more than two oscillations occur before returning to baseline.
The system is underdamped which may be caused by:
- Catheter whip or artefact
- Stiff non-compliant tubing
- Hypothermia
- Tachycardia or dysrhythmia

Importantly, systole would appear falsely high and diastole falsely low.
If there are no oscillations after the square wave, or the response is sluggish, the system is overdamped. Causes can be:
- Loose connections
- Air bubbles
- Kinks
- Blood clots

Importantly, systolic values can be underestimated and diastolic overestimated.
- At set up of arterial line and prior to using EDM+
- At handover
- Whenever you are unsure of the arterial readings
- If the arterial line is disconnected from the patient monitor.
- Arterial spasm
- Narrow tubing
Parameters
Click parameter to see definition

The data boxes can be customized when switching the monitor on by pressing ‘Monitor settings’ and then ‘User settings’. Use the large ‘Control knob’ to identify and select the parameter for each box.

